

The NWT is proposing changes to the benefits system that covers people who can’t access health coverage through work or other forms of government insurance.
The proposal only applies to a specific group: seniors are excluded, as is anyone Indigenous who qualifies for federal Non-Insured Health Benefits or territorial Métis Health Benefits.
The NWT government estimates that leaves 2,200 NWT residents with no access to benefits. The territory says its proposal “will ensure all residents in need of health benefits can get them.”
The proposal uses income testing to determine how people are helped to pay for prescription drugs, eyewear, dental treatment, medical equipment and some medical travel – things basic NWT health coverage does not cover.
Advertisement.
Advertisement.
But critics say the territory is glossing over the way in which its proposal would take benefits away from some people with serious existing conditions.
Specifically, the territory is proposing to do away with what is currently called the Specified Disease Conditions Program. The program guarantees coverage if you have a serious or chronic condition on the program’s list and can’t cover the costs through another form of insurance.
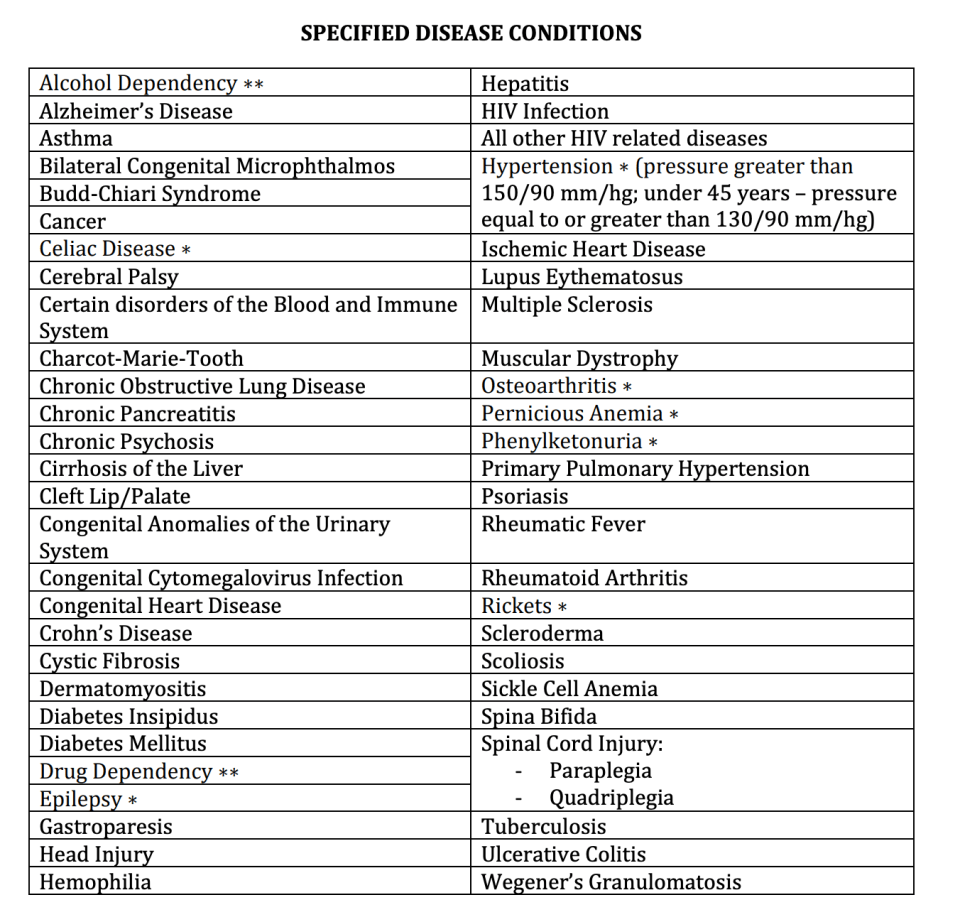
Stacy Ridgely is the Department of Health and Social Services’ director of policy, legislation and communications. Ridgely says the Specified Disease Conditions Program is too narrow, and that’s why things need to change.
“We have a list of specified diseases but not everybody that requires assistance has those specified diseases,” Ridgely told Cabin Radio.
Advertisement.
Advertisement.
“It’s a backwards way of providing some sort of social safety net.
“The work that we’re doing is to flip it so that we are actually creating a benefit program that’s based on equity and access, so it doesn’t matter whether you have a diagnosis for something. Whether you can pay for it, that’s the point of it.”
The problem comes in the way that the new system works.
Some people who have conditions listed in the Specified Disease Conditions Program say they’ll lose out in the new system because treatments previously covered in full will now require them to get health insurance – which can be expensive if you have an existing condition – and pay premiums and co-payments until they reach a certain threshold, after which some help with costs will be provided.
Rylund Johnson, the MLA for Yellowknife North, expressed concern that the GNWT’s communication of the proposals included various cartoon images setting out the ways in which people would benefit from the new-look program, but did not communicate any of the situations in which people may have their coverage reduced.
“I’m not sure if it was intentional or just misguided,” said Johnson, “but they really did not explain to people who are in that current schedule of pre-existing conditions that they would be potentially losing their benefits.
“If you’re going to draw little cartoons to explain it, maybe you should draw the one where the guy making $45,000, currently holding on to his job and getting cancer treatment, is about to lose his coverage.”
Proposal ‘not finalized’
Cancer treatment is a source of confusion. Cancer is listed in the Specified Disease Conditions Program, and that program is scrapped under the proposal in favour of income testing. But Ridgely insisted coverage related to cancer is not part of this conversation.
Advertisement.
Advertisement.
“Cancer is a tricky one because cancer is an insured health service. So it wouldn’t be part of this,” Ridgely said.
Johnson says he has spoken with the NWT’s health minister and that isn’t his understanding of how cancer patients who don’t have any other coverage would be affected.
“Assuming they don’t [fall below] the income threshold, they will lose their benefits,” he said, describing his understanding of what would happen to such a patient. “They will be required to go get private health insurance first, which is an extremely difficult thing to do if you are in the midst of cancer treatment, then exhaust $3,000 worth of drug benefits under that private policy that they got, and then possibly be able to go back to the GNWT.”
Amid this confusion, a little over two weeks remain before the window closes for feedback through the GNWT’s Have Your Say website.
“We put together a straw dog – for lack of a better term – for people to look at, to push up against, and to see how that sat with them,” said Ridgely.
“It has not been finalized by any stretch of the imagination. All we want to do is to have people weigh in. How do you feel about this?
“Yes, it will affect some people but it will also positively affect some people as well. It’s hard to talk about the people that it’s going to negatively affect when you have to look at how many people it’s going to positively affect as well.”
Below, read our full interview with Ridgely regarding the impact of the proposal on certain groups of people. You can also read the GNWT’s discussion paper about the proposal, which sets out why the NWT government believes the suggested changes are beneficial.
Advertisement.
Advertisement.
After the Have Your Say feedback window closes on October 14, you can still send feedback to Ridgely and the GNWT team working on the proposal by email.
This interview was recorded on September 26, 2022. The transcript has been lightly edited for clarity.
Ollie Williams: What do you think the key changes are here?
Stacy Ridgely: What we’re trying to do with this engagement is to validate the development of good public policy. Our current model, under the Extended Health Benefits policy, is unsubstantiated. We have a list of specified diseases but not everybody that requires assistance has those specified diseases, so it’s sort-of a backwards way of providing some sort of social safety net. The work that we’re doing is to flip it so that we are actually creating a benefit program that’s based on equity and access, so it doesn’t matter whether you have a diagnosis for something. Whether you can pay for it, that’s the point of it.
For instance, we have folks that are working three jobs but none of them have a benefit package and they need to have a prescription filled for antibiotics. When you’re living hand-to-mouth, do you feed your kids or do you get your antibiotics? What we’re doing is looking at providing that social safety net, providing equity of access to these really important drug benefits, dentistry and that sort of thing. A number of people haven’t got access right now through the employer plan.
Why is income testing considered the way forward?
Income testing determines need and that’s the model used across Canada. How do you provide these benefits to people without leaving out other people or providing benefits to a group of people and not providing them to someone else?’ The only way to really do that is by income testing. Now, we can provide without discrimination because it’s based on need, not on who you are, what you are, or any of those other things.
This is billed by the GNWT as an expansion of benefits. In what circumstances would people have less coverage under this proposal than is currently the case?
Advertisement.
Advertisement.
It is the people that are currently covered under the Specified Disease Program. Depending on where they fall on the income testing, they may not get full coverage. They may be asked or may be required to have a cost-share.
Do you know how many people the GNWT estimates that would affect?
Absolutely no idea. We know how many people are on the specified disease list but it wouldn’t necessarily affect them all, and it certainly wouldn’t affect them in the same way. So it’s hard to attach a number to it.
Part of why we’re doing this public engagement is to validate the policy. Once the program is designed and decisions are made around income thresholds, we can start putting numbers around how many people this might affect and how that income threshold will affect people. None of those decisions have been made.
In our public engagement, we put together a straw dog – for lack of a better term – for people to look at, to push up against, and to see how that sat with them. It has not been finalized by any stretch of the imagination. All we want to do is to have people weigh in. How do you feel about this? Yes, it will affect some people but it will also positively affect some people as well. It’s hard to talk about the people that it’s going to negatively affect when you have to look at how many people it’s going to positively affect as well.
How many people will it positively affect?
Well, we don’t know. The only way we can figure that out is by deductive reasoning. We know how many GNWT employees there are. We know how many people are on NIHB. We know how many people are on Metis health benefits. We know how many seniors we have. So it’s basically deducing from how many people that we know have insurance as opposed to the people that we don’t know.
I’m going to read an example out to you. You tell me if this is your understanding of how this new system would work.
Advertisement.
Advertisement.
Here’s the example, which was provided by an NWT resident concerned about the impact of the proposed changes:
Let’s say I’m self-employed and I have a child with cancer. At the moment, the cost of treating that cancer would be covered under the Specified Disease Program. Under these changes, I would need to find a health insurer first, sign up for a plan that involves a pre-existing condition, pay the premiums for that, and pay the co-payments for the child’s treatment. Once I’ve paid a portion of my income annually, I would be able to apply for some coverage for the rest of the cost.
Is that an accurate understanding?
Well, cancer is a tricky one because cancer is an insured health service. So it wouldn’t be part of this.
Why would cancer not be a part of any of this?
When you get cancer treatment, it’s paid for by the government because it’s not a prescription drug.
But drugs are sometimes involved in treating cancers.
They’re covered under your NWT healthcare card.
Advertisement.
Advertisement.
OK, so nobody with cancer in the NWT need worry about these changes?
That’s correct.
OK. HIV?
Well, I’m not sure. It depends. I’d have to look that up. There’s a whole other world of clinical decision-making about what’s covered under our NWT healthcare plan versus what’s not, so I would have to look into that to find out. If you don’t have an employer plan, then we would go to the income testing model. If it’s a prescription then yes, it would fall under this. You would be income tested. If you had an employment plan and you exhausted your employment plan, then you would apply to this and you would go through the income-testing process to see where you landed on the schedule and go from there.
At the very least, it sounds like it might be more confusing for some people under the new plan than the old one.
Oh, absolutely. Change is always confusing. That’s kind-of par for the course. While we work through it and we guide people through the process, it will become normal.
Will there be anywhere people can go to understand how, under this proposal, their specific condition would be affected?
At this point, we’re just talking about building the policy and validating the principles of the policy. As we move through this, there will be more opportunities to have people put their information into a tool to find out what their coverage will be.
Advertisement.
Advertisement.
And that tool will be available before final decisions are made so people can feed back?
Yes.
Do you have an idea of the estimated change in overall cost to the GNWT of this proposal?
No. I know the costing will be important, and it will come. Right now, there needs to be some recognition that by changing this – and supporting people that don’t have coverage at the moment and providing benefits that end up being preventative in nature – we’re also looking at the downstream costs of acute care services that are delivered at the hospital. By investing in the front end, we’re going to reduce visits to the ER, that sort of thing. When a person hasn’t had access to prescription drugs or to dental care, they suddenly end up at the ER. That’s what happens now, and it’s a very expensive way to deliver services.
Trying to put a price on those things is a big piece of work, which we’re going to get to – we just haven’t got there yet, because we wanted to ensure that we were designing a program based on solid policy, and then we’ll do the costing. So it’s coming.
Will there be an opportunity for people to develop their understanding of this policy before they feed back about it?
Well, we have to go through government processes. So it will go to the Standing Committee on Social Development, and they often take things to the public. There has to be a lot of feedback through all of those channels. After we finish our public engagement we’ll have our What We Heard report, which will then go up through cabinet to the standing committees and what have you. Through those processes, there are always opportunities for the public to weigh in.
Given the importance of that tool you just talked about, is this public feedback stage closing a little early?
Advertisement.
Advertisement.
Not necessarily. With our focus just being on validating the public policy development and making sure that we’re in the right ballpark, that we’re doing the right thing, that’s very important. This work has been ongoing for a number of years – way before my time – and there have been some pitfalls along the way and we have been very careful in how we move forward, because it is a very complex subject and there are a lot of moving parts, so just taking it step by step and not rushing ahead before we have the foundation worked on. It hasn’t been a success in the past because things went too quickly and people didn’t understand all of the nuances and complexities around this kind of work. It’s not simple. If it was simple, we would have fixed it a long time ago.
After October 14, if it heads into the legislative process at that point, how do people feed back?
Send things to us. We’re closing part of the engagement but people can always get in touch with us. Our email box will remain open until we’ve finished this entire process.